About the research
The continuing rise in life expectancy has been linked to an increase in the number of
people diagnosed with dementia. Britain’s ageing population means that within
three years, more than a million people will have dementia, despite a fall in the individual risk factors such as smoking and
cardiovascular disease. It is known that
lower socioeconomic status is associated
with increased risk of many serious illnesses, but the evidence concerning
dementia is mixed. The research team, therefore, assessed in a longitudinal
study, multiple facets of socioeconomic position in relation to dementia. Individual factors contributing to an
individual’s socioeconomic position such
as education and wealth were reviewed, as well as the deprivation level of the
area in which participants lived.
The research found that wealth in later life, but not educational attainment, was associated with an
increased risk for dementia. These
findings demonstrate that older adults in England with fewer financial
resources are more likely to develop dementia, even when controlling
statistically for age, gender, marital status and health.
No substantive differences were
identified in relation to the area
of neighbourhood deprivation. The findings
indicate that the person’s own economic
resources, not the area in which they live are significant. An age-cohort
effect was observed, highlighting that socioeconomic inequalities were more
robust among people born more recently. The
association was more consistent for participants born after 1926, compared with
those born earlier in the 20th century. Furthermore, there was evidence
for a reduced incidence of dementia among
participants born more recently but who had increased socioeconomic
inequalities.
There are several possible explanations for the strong
relationship between wealth and subsequent health outcomes. Wealth is an
indicator of socioeconomic resources, and
could represent a gateway to more mentally and socially stimulating
environments, independent of the level of education. Previous research using
ELSA has shown that increased wealth
facilitates greater digital literacy, which is in turn associated
with a reduced risk of dementia. Furthermore, increased financial status could
provide broader access to cultural resources and behaviours (reading, theatres,
social clubs), increased social networks, ultimately contributing to higher
cognitive reserve.
Methodology
Data from the English Longitudinal Study of Ageing (ELSA) were used in the research. ELSA is a prospective cohort study that is representative of the English population. Dementia was determined by physician diagnosis and the Informant Questionnaire on Cognitive Decline in the Elderly.
The researchers were also interested in investigating the change in dementia incidence rates during the last decade from 2002 to 2014,and therefore derived two independent groups for all participants aged 65 years and older at baseline interviews, in those born between 1902-1925 and 1926-1943.
Given that death is often considered a competing risk for dementia incidence, supplementary analyses were also conducted to account for the competing risk of death.
Socioeconomic status was measured using individual-level (education and wealth) and area-based characteristics at baseline interview (measured at the first wave of data collection for each participant).
Educational attainment was classified into four categories:
1. university degree or higher;
2. A-levels or equivalent, comparable to high school graduation
3. below A-level;
4. no formal qualifications.
Wealth was calculated by summing wealth from property,possessions, housing, investments, savings, artwork, and jewellery, and net of debt and divided into quintiles. The Index of Multiple Deprivation was used, which represents a composite measure which combines multiple area-level of deprivation indicators into a single overall score. The official measure from 2004 for England were also used and grouped into quintiles (1= least deprived).
In this study, there was a more detailed assessment of wealth than is available in most studies to date, since the measure was computed on the basis of accurate information on multiple individual components, rather than broad categorisation of assets. Through the extensive monitoring of biennial interviews and a long-term follow-up, an integrative approach to study the association between various socioeconomic factors and dementia incidence could be used.
In the sample of 6,220 individuals, aged 65 and older at study entry, there were 463 new cases of dementia ascertained over 12 years follow-up from 2002-2003 until 2014-2015. The baseline median age for the entire sample was 73 years, while the median age at the time of dementia ascertainment was 83. The sample was 55% female, 59%married, and 53% had no formal educational qualifications. Only 17% of participants attended university. More men were educated to university degree level than women, while more women had no formal educational qualifications.Age and sex-adjusted incidence rates for the full ELSA sample are presented in Figure 1.
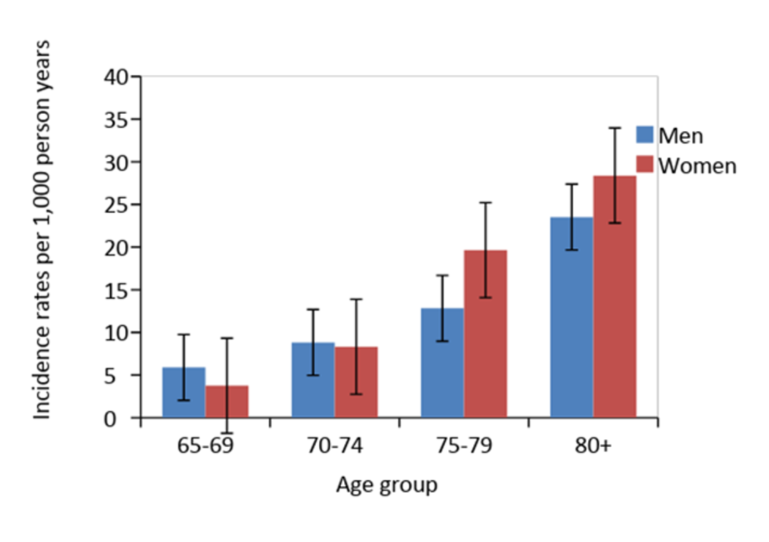
Figure 1. Dementia incidence rates per 1,000 person-years presented by age-groups and gender in ELSA (click for larger version)
As anticipated, there was a significant increase in dementia incidence rates with age from 4.38 in people aged 65-69 years to 24.69 for those aged 80+ years. The findings indicate the incidence of dementia incidence is almost double with every five years increase from the age of 65 years.
Additional analyses considering the competing risk of death showed a slight decline in dementia incidence over time, among participants born more recently (see Figure 2).
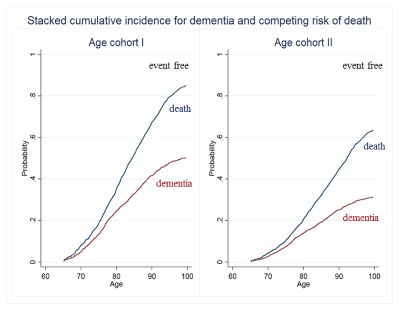
Figure 2. Hazard risks of dementia by age within each age cohort I & II in ELSA,taking in consideration the competing risk of death
However, the two age-cohorts overlap only for the 75-79 age groups and the differences between age-cohorts in the incidence of early versus later onset dementias may also be present. However, the researchers were not in the position to investigate those differences.
In the overall ELSA sample, education was not significantly associated with dementia incidence, but wealth was a strong indicator of dementia incidence.
The risk of developing dementia was higher for those in the lowest wealth quintile compared with those in the highest, independent of education, the area of deprivation and health indicators (see Figure 3).
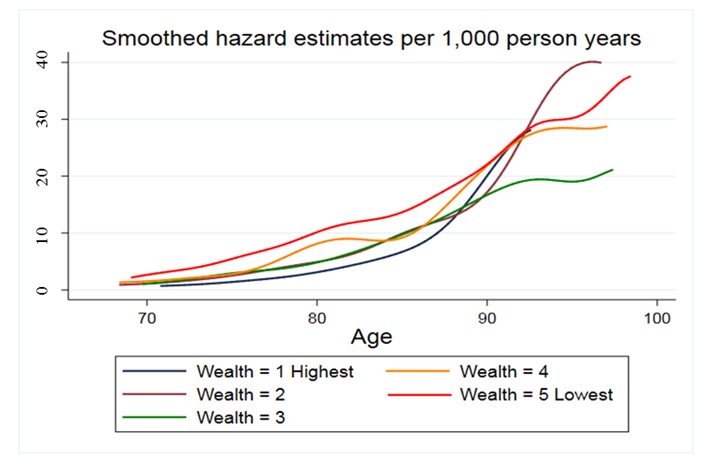
Figure 3. Hazard risks of dementia calculated by age and wealth quintiles (per 1,000 person-years) in ELSA (click for a larger version)
The findings suggest a higher risk for individuals with fewer financial resources. The association was more consistent for participants born after 1926, compared with those born earlier in the 20th century. There are several possible explanations for the strong relationship between wealth and subsequent health outcomes. Increased financial status could provide broader access to cultural resources and behaviours (reading, theatres, social clubs), increased social networks, ultimately contributing to higher cognitive reserve and mental resilience, independent of the level of education.
It is also possible that individuals born before World War II may not necessarily have been able to access higher education (due to military service, financial restrictions and limited university place availability), but may have gained access to intellectually challenging jobs and growth financial opportunities after the war.
The lack of a contextual area-based socioeconomic impact on dementia incidence was also notable. Previous research using ELSA has documented a link between neighbourhood deprivation and cognitive functioning,independent of individual markers of socioeconomic status, showing that individuals living in the most deprived area of England had significantly lower cognitive scores compared with those living in the most affluent regions. The study found an inconsistent association between area deprivation and dementia incidence, suggesting that much of the effect of area deprivation is explained by the characteristics of the people living in those areas, rather than features of the areas themselves. The reasons are not clear, but it may be concluded that less affluent people were at higher risk of dementia. However, the findings cannot be attributed to a person’s education or cardiovascular risk factors such as high blood pressure since they were controlled for in the research methodology.
Findings for policy
In an English nationally-representative sample of people
aged 65 years and older, the risk of dementia incidence was associated with socioeconomic indicators, most notably wealth.
Socioeconomic inequalities were more marked in individuals born in later years
(from 1926 onwards) than in those born earlier.
Public health strategies for dementia prevention should identify
and target the existing socioeconomic
gaps to reduce health disparities and protect those who are particularly
disadvantaged, in addition to addressing vascular risk factors such as
hypertension, diabetes mellitus, smoking, and heart disease.
Impact
Given that education is typically completed many decades before dementia onset, other individual and area-based components of socioeconomic status, such as wealth, income and area deprivation may provide a more accurate indication of current socioeconomic resources in any contemporary cohort of older adults. Increased financial status seems to indirectly protective against chronic disease in older age by providing access to greater digital literacy, healthier lifestyle,broader access to cultural resources and behaviours (reading, theatres, social clubs), which ultimately contribute to a higher mental resilience in older adults.
It is imperative that a multi-integrative society is created that supports mental activities and stimulating social networks for older people, who may not have benefitted from educational opportunities in early life, in order to promote their physical and mental resilience until later in life.
The research has had wide media coverage. Just over 40 websites have covered the research, including UK newspapers such as The Guardian and the Daily Mail and international new outlets such as the NewIndian Express. The research has been cited by the American Psychiatric Association and has been referenced on a range of medical and health websites including WebMD.
There have been 180 tweets about the research including positive commentary from the Northern California Psychiatric Society,a researcher at the Centro de Salud Cerebral (Centre for Brain Health) at the University of Buenos Aires and IntraMed (a Spanish-speaking medical community on the internet).
Read the full article
Individual and Area-Based Socioeconomic Factors Associated With Dementia Incidence in England: Evidence From a 12-Year Follow-up in the English Longitudinal Study of Ageing
Funding
Funding/Support: The work was
supported by the National Institute on Aging (grants 5218182,
RO1AG7644-01A1, and RO1AG017644). The English Longitudinal Study of Ageing is
funded by the National Institute on Aging (grant RO1AG7644) and by a consortium
of UK government departments coordinated by the Economic and Social Research
Council (ESRC) and the Office for National Statistics. Professor David Batty is also supported by the UK Medical Research Council.
Role of the Funder/Sponsor: The funders had no role in the
design and conduct of the study; collection, management, analysis, and
interpretation of the data; preparation, review, or approval of the manuscript;
and decision to submit the manuscript for publication.
Related articles and publications
- Most
deprived are more likely to develop dementia (from UCL News site) - Media
coverage of the research (from UCL News site) - Cohort
profile: the English longitudinal study of ageing
Studies