About the research
The recent
2018 Intergovernmental Panel on Climate Change (IPCC) Special Report highlights the speed and urgency with which action must be taken to prevent global warming exceeding 1.5 degrees Celsius. A reduction of energy demand through behaviour change will be an important element in tackling climate change. An important question is which groups of people might find it difficult to save more energy due to their life circumstances? Which groups would be at a disadvantage if climate change mitigation policies make energy more expensive?
The research focused on how people’s health might influence their ability to save energy, with three main research questions:
- Is health an important factor in people’s ability to save energy in addition to factors such as age and income?
- Do people living with health challenges use more energy in the home but travel less owing to health related mobility challenges? The “mobility hypothesis” may indicate that people living with health challenges would be disadvantaged by rising electricity and gas prices or taxes.
- As it is well-established that people living with health challenges also tend to have lower incomes, a factor which is associated with less home energy use and travel; do people living with health challenges use less energy and travel less (“income hypothesis”)?
Funding for the research
The research was funded by the UK Engineering and Physical Research Council (EPSRC) grant “Transforming the Engineering of Cities to Deliver Societal and Planetary Wellbeing” (EP/J017698/1).
Key messages
The research findings show people living with health challenges using more electricity and travelling less than people not experiencing health challenges. The research explores how limited mobility rather than low income may be an important factor in energy usage. People living with health challenges may be disadvantaged by taxes on home energy and additionally, may have unmet travel needs. The findings indicate an opportunity for low carbon public transport options to be made more accessible and affordable for people living with health challenges.
Methodology
The Understanding Society study, or the United Kingdom Household Longitudinal Study (UKHLS), which began in 2009, is conducted by the Institute for Social and Economic Research (ISER), at the University of Essex. As a multi-topic household survey, the purpose of Understanding Society is to understand social and economic change in Britain at the household and individual levels. It is anticipated that over time the study will permit examination of short- and long-term effects of social and economic change, including policy interventions, on the general wellbeing of the UK population.
The Understanding Society study is a successor to the
British Household Panel Survey (BHPS). The BHPS sample forms part of Understanding Society from Wave 2 onwards.
The
2012-14 wave of Understanding Society was used for the research because it covers a broad range of questions about people’s environmental attitudes and behaviours (which are repeated in every 4th wave), as well as questions on their self-reported health status. There is no other representative UK survey with a similar sample size which covers all of these questions. The sample consisted of nearly 47,170 individuals in just over 25,800 households.
Some of the survey variables were used to estimate households’ actual energy use. For instance, price data on gas and electricity was applied to estimate kWh consumed, based on households’ gas and electricity expenditure.
To estimate kWh related to car travel, information on annual car miles per household from Understanding Society was utilised. To these data a factor of kWh per mile, derived from government statistics on total household car miles travelled and the total calorific value associated with this travel, was applied.
Information on air travel is captured by the number of annual flights per person. Public transport as well as walking and cycling are covered by questions on the frequency with which individuals engaged in these modes of travel.
Bivariate and multivariate analysis was conducted to examine relationships between people’s health status and their energy use.
People’s self-assessed health was captured on a scale from 1 to 4 where 1 is ‘excellent/very good’ and 4 ‘poor’. The multivariate regression models (using ordinary least squares for direct energy use, and logistic regression for a range of other travel modes) controlled for age, income, household size and presence of children, education, economic activity, gender, rural/urban location, and environmental attitudes.
The relationship between people’s health and their energy use was examined in two ways, firstly unconditionally, without controlling for other household or individual characteristics, and secondly conditionally, taking household and individual characteristics into account.
Data used from the UK Data Service collection
Messages
The research findings show people living with health challenges using more electricity and travelling less than people not experiencing health challenges. The research explores how limited mobility rather than low income may be an important factor in energy usage. People living with health challenges may be disadvantaged by taxes on home energy and additionally, may have unmet travel needs. The findings indicate an opportunity for low carbon public transport options to be made more accessible and affordable for people living with health challenges.
Findings
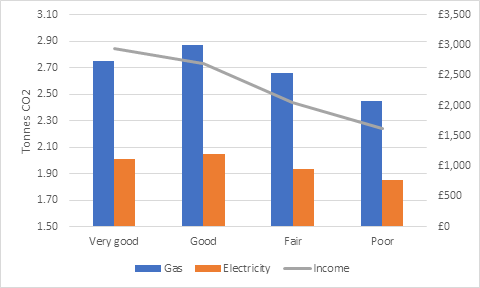
The research found that people who self-assessed their health as ‘poor’ used less energy in the home, as well as when travelling, compared to people who self-assessed their health as ‘good/excellent’ in the survey. The finding supports the hypothesis that income is the main factor for explaining differences between people who self-assessed their health as poor and good in the survey. Since people living with health challenges may also tend to be on lower incomes, they might try to save on gas, electricity and motor fuels, and not be able to afford as many train rides and flights as people with higher incomes.
Figure 1: Annual emissions from electricity and gas, and monthly household income over health status
Source: Understanding Society Wave 4 (2012/3)
However, once income, age, presence of children, employment status and other characteristics are controlled for, people who self-assessed their health as ‘poor’ use significantly more electricity in the home than people who self-assessed their health as excellent/very good’.
Taking two households which both have the same income, average age, number of children, etc., the household whose members rated their health as ‘poor’ used more electricity. In all other areas, households whose members rated their health as ‘poor’ still used the same amount of energy (gas) or less amount of energy (travel). Thus, there is some evidence for the ‘mobility’ hypothesis that different energy use of people in self-assessed ‘poor’ and good/excellent health may be explained by different capacities for mobility: people in who self-assessed their health as poor seem less able to move around outside their homes, and hence use more electricity than their counterparts, regardless of their other circumstances.
It is interesting that the same evidence for gas use was not found. One explanation for this finding could be that people who are “stuck at home” might be able to find ways of saving on heating, e.g. by putting on more layers, whilst their capacity for limiting electricity use might be more limited – they will have to switch the light on when it is dark, and many will use electronic devices for entertainment purposes.
Not unsurprisingly, it was also discovered, in both steps of the analysis, that people who self-assessed their health as poor participate less than people who self-assessed their health as ‘good/excellent’ in environmentally friendly types of travel such as walking, cycling or public transport. Likely explanations may be a combination of:
- limited physical mobility, especially for walking and cycling
- financial constraints – travel on public transport can be expensive on certain routes and in particular areas
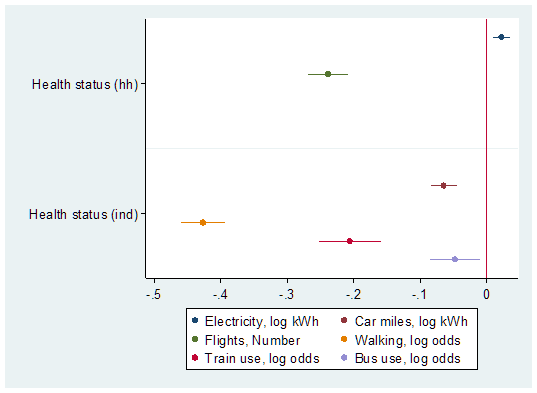
Figure 2 – Regression coefficients for health status
Note: The regression coefficients for health status are not directly comparable because they refer to different models, however, they do demonstrate the divide between electricity and travel. Electricity is significantly higher for people in poor health, while travel is notably lower for both high and low carbon modes for people in poor health, compared to healthier people.
Findings for policy
The research findings have important policy implications:
- Poor health may put people at a disadvantage in relation to saving electricity or using environmentally friendly means of travel compared to people in better health, for given income levels and other characteristics.
- People in poor health may be negatively affected by rising electricity prices or taxes.
- People in poor health might have travel needs that they find difficult to meet due to financial and mobility constraints.
People in poor health may, however, tend to be less affected by eco-taxes on motor fuels or flights than healthier people because they spend a smaller proportion of their incomes on these services compared to healthier people. Improving the population’s health could not only increase engagement in low carbon modes of travel, but also their more environmentally damaging counterparts. Therefore, accompanying measures are required to dis-incentivise car and air travel which would cut emissions while putting less of a burden on people in poor health, so public transport systems need to be made more accessible and affordable.
Finally, policies should aim not to unfairly burden people for types of energy use that they have little control over, but rather focus on discretionary or “luxury” types of energy use.
Impact
The research received coverage on social media and has been cited in 4 other academic papers.
Publications
Related research
- Büchs, M. and S. V. Schnepf (2013). “Who emits most? Associations between socio-economic factors and UK households’ home energy, transport, indirect and total CO2 emissions.” Ecological Economics 90: 114-123. https://doi.org/10.1016/j.ecolecon.2013.03.007
- Büchs, M., et al. (2014). Unequal emissions – unequal policy impacts: how do different areas of CO2 emissions compare? International Handbook on Social Policy and the Environment. T. Fitzpatrick. Cheltenham, UK, Edward Elgar: 62-92. https://eprints.soton.ac.uk/id/eprint/364955
- Buchs, M., et al. (2011). “Who bears the brunt? Distributional effects of climate change mitigation policies.” Critical Social Policy 31(2): 285-307. https://doi.org/10.1177%2F0261018310396036